

Why Generic Prescribing Isn't Just About Saving Money
When you write a prescription, you're not just choosing a drug-you're choosing a system. Generic prescribing means writing the drug's international non-proprietary name (INN), like atorvastatin, instead of the brand name Lipitor. It sounds simple, but it's one of the most powerful tools doctors have to cut costs, reduce errors, and improve patient outcomes. And it's not a suggestion-it's now standard practice in most healthcare systems.
The NHS in England estimates that switching to generic prescribing saves £1.3 billion every year. In the U.S., generic drugs saved the system $313 billion in 2019 alone. These aren't theoretical numbers. They're real savings that free up resources for other care. But the real benefit isn't just financial. Generic prescribing reduces confusion, cuts down on medication errors, and helps patients stick to their treatment plans because they can afford it.
How Generic Drugs Are Proven to Work the Same
Many patients worry: "Is the generic version really the same?" The answer is yes-when it's approved by regulators. The FDA, EMA, and MHRA all require generics to meet strict standards. A generic drug must contain the same active ingredient, in the same strength, dosage form, and route of administration as the brand. It must also be bioequivalent: meaning it delivers the same amount of medicine into the bloodstream at the same rate.
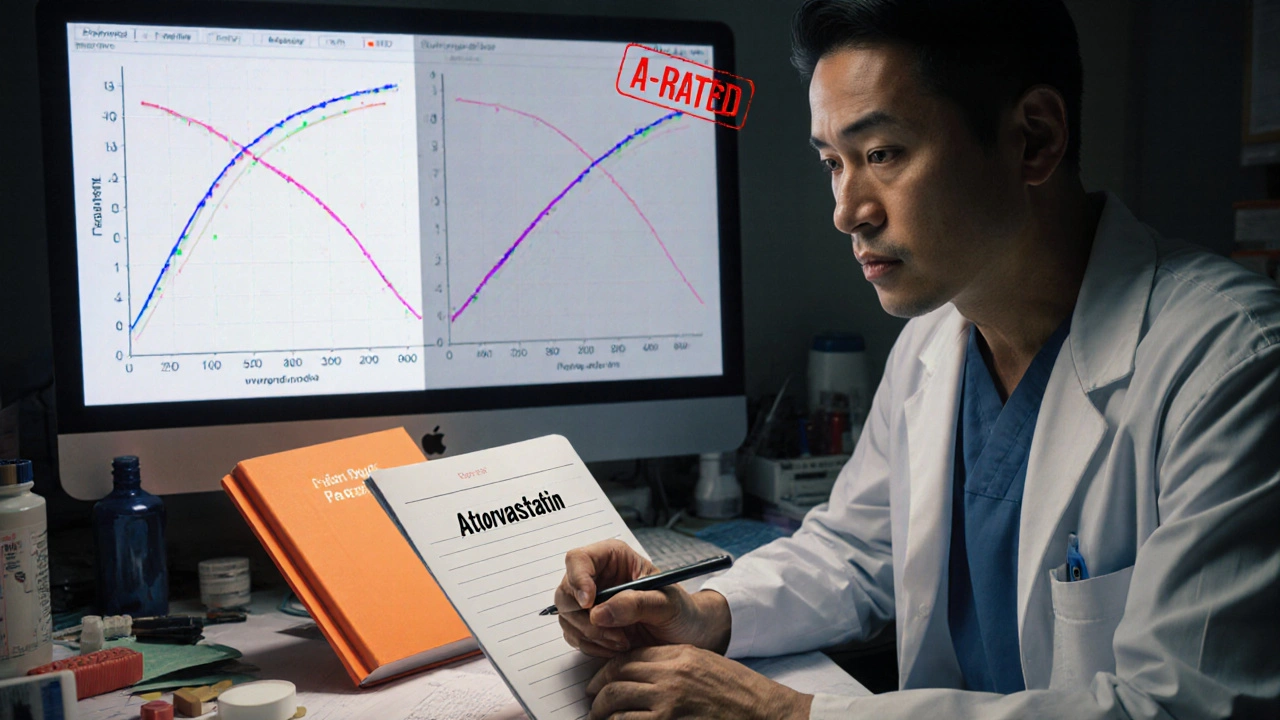
The FDA requires generics to show 80-125% bioequivalence compared to the brand. That’s not a wide range-it’s tight enough to ensure consistent effects. For example, generic atorvastatin and brand-name Lipitor have the same blood concentration curves. The same goes for omeprazole versus Losec. The inactive ingredients (fillers, dyes) might differ, but those don’t affect how the drug works.
Every approved generic is listed in the FDA’s Orange Book with an "A" rating, meaning it’s therapeutically equivalent. In the UK, the British National Formulary (BNF) does the same. These aren’t just opinions-they’re backed by clinical data from thousands of patients.
When You Should Still Prescribe by Brand Name
Generic prescribing is the default. But not the only option. There are specific cases where brand-name prescribing is necessary. The BNF identifies three categories where switching can be risky:
- Category 1: Narrow therapeutic index drugs-These have a small window between effective and toxic doses. Examples: warfarin, levothyroxine, phenytoin, carbamazepine, digoxin. Even small changes in absorption can cause serious problems. For warfarin, switching brands can lead to dangerous INR fluctuations. For levothyroxine, patients stabilized on one brand often do worse after switching.
- Category 2: Modified-release formulations-Drugs like theophylline ER or extended-release methylphenidate. The way the drug is released matters. Generic versions may use different polymers or coatings, leading to inconsistent absorption. Pharmacists report these are the most common cause of substitution problems.
- Category 3: Biologics and biosimilars-The MHRA and FDA both require brand-name prescribing for biologics like adalimumab or rituximab. These are complex molecules made from living cells. Switching between originator and biosimilar can trigger immune reactions. Unlike small-molecule drugs, biosimilars aren’t interchangeable by default.
That’s about 2% of all prescriptions. But it’s critical to know which ones they are. Many prescribers forget the exceptions-especially when switching from brand to generic in long-term patients.
Why Patients Resist-and How to Fix It
Most patients don’t care about the name on the bottle. But some do. A 2022 NHS survey found 34% of GPs worried about patient pushback when switching to generics. Why? Because of the nocebo effect-the opposite of placebo. If a patient believes the generic is inferior, they’re more likely to report side effects or lack of effectiveness-even when there’s no difference.
Studies show that when doctors explain the switch, acceptance jumps from 67% to 89%. Here’s what works:
- "This is the same medicine as your old pill. The active ingredient is identical. It’s just cheaper."
- "It’s been tested in thousands of people. The FDA says it works the same."
- "You’ll save about £12 a month. That’s £144 a year."
Don’t say, "It’s just a generic." That sounds dismissive. Say, "This is the same drug, approved by the same regulators, just without the brand name."
Some drugs get more complaints than others. Sertraline and levothyroxine are common trouble spots. Patients report feeling "off" after switching-even when lab tests show no change. That’s not always a real problem. It’s often anxiety. But you still need to listen. For these patients, staying on the same brand may be worth the cost.
How to Make Generic Prescribing Routine
Getting to 90%+ generic prescribing isn’t hard-it just takes structure. NHS England’s 2023 toolkit outlines four steps:
- Audit your prescribing-Use your practice’s prescribing dashboard. See what percentage of your scripts are generic. Compare to your peers.
- Train your team-Make sure everyone knows the three exception categories. Post the BNF list where you write prescriptions.
- Set electronic defaults-Most e-prescribing systems let you set generic as the default. Turn it on. Only override when necessary.
- Monitor and adjust-Track your rates monthly. If you’re at 85%, what’s holding you back? Is it patient complaints? Unclear exceptions? Fix the gap.
New prescribers usually hit 90%+ within 2-3 months. The hardest part isn’t knowing the rules-it’s remembering them under pressure. Keep the BNF exception list handy. Use it like a checklist.

What’s Changing in 2025
Generic prescribing isn’t standing still. The MHRA updated its guidance in March 2023 to include complex generics like glatiramer acetate-drugs with tricky manufacturing processes. These now require brand-name prescribing because even small changes can affect how they work.
The FDA’s GDUFA III rules, rolled out in 2023, require generic manufacturers to report adverse events tied to formulation differences. That means we’ll see better data on when generics cause real problems-not just perceived ones.
By 2025, 75% of small-molecule drugs will have generics. But biologics? Only 40% will have biosimilar options. And even then, they’ll still need to be prescribed by brand name. The future isn’t about eliminating brands-it’s about smart substitution. Use generics where they’re safe. Stick with brands where they matter.
Bottom Line: Prescribe Generically-Unless There’s a Clear Reason Not To
Generic prescribing isn’t a cost-cutting gimmick. It’s evidence-based medicine. It reduces errors, improves adherence, and saves billions. Most patients do just fine on generics. The exceptions are real-but they’re rare.
Your job isn’t to avoid generics. It’s to know when they’re safe and when they’re not. Use the BNF and FDA guidelines as your anchors. Educate your patients. Set your systems to default to generic. And when in doubt-stick with the brand.
It’s not about being cheap. It’s about being smart.
Are generic drugs really as effective as brand-name drugs?
Yes, for the vast majority of drugs, generics are just as effective. Regulatory agencies like the FDA and EMA require generics to prove they deliver the same active ingredient at the same rate and amount as the brand. Bioequivalence studies show no clinically meaningful difference in how the drug works in the body. Thousands of studies and real-world data confirm this. The only exceptions are narrow therapeutic index drugs, modified-release formulations, and biologics-where even small changes can matter.
Why do some patients say generics don’t work for them?
Often, it’s the nocebo effect-when patients believe a generic is inferior, they experience side effects or reduced effectiveness even when there’s no real difference. Studies show that when patients are properly educated about generics, complaints drop by over 30%. Some drugs, like levothyroxine or sertraline, have more patient-reported issues, but lab results usually show no change. For these cases, consistency matters: if a patient is stable on a brand, switching may do more harm than good.
Which drugs should never be switched to generic?
The British National Formulary (BNF) identifies three key categories: 1) Narrow therapeutic index drugs like warfarin, levothyroxine, phenytoin, and carbamazepine-where small changes in blood levels can cause harm; 2) Modified-release formulations like extended-release theophylline or methylphenidate, where the release mechanism may differ between brands; and 3) All biologics and biosimilars, which must be prescribed by brand name to prevent immune reactions. These represent about 2% of prescriptions but require special attention.
Does prescribing generics reduce medication errors?
Yes, significantly. With generics, each drug has one standardized name (e.g., amlodipine). Brand names vary by manufacturer-amlodipine might be sold as Norvasc, Amvaz, or Katerzia. This reduces confusion for pharmacists, nurses, and patients. The Institute for Safe Medication Practices found generic prescribing cuts medication errors by up to 50% by eliminating brand-name ambiguity.
How can I increase generic prescribing in my practice?
Start by setting your electronic prescribing system to default to generic names. Audit your current prescribing rates using your practice’s dashboard. Educate your team on the three exception categories using the BNF guidelines. Use simple, clear language to explain the switch to patients: "This is the same medicine, just without the brand name. It’s cheaper and works the same way." Most practices reach 90%+ generic prescribing within 6 months.
Do generic drugs have lower quality?
No. Generic manufacturers must meet the same quality, purity, and potency standards as brand-name companies. The FDA inspects generic facilities just as rigorously. In 2021, the FDA found only 12.7% of generics had minor deviations from specifications-none affected safety or efficacy. Manufacturing shortages happen, but they’re usually due to supply chain issues, not quality problems. Quality isn’t the issue with generics-it’s consistency in specific cases like modified-release or complex drugs.
What to Do Next
If you’re not already prescribing generics by default, start today. Check your prescribing dashboard. Look at your top 10 most prescribed drugs. Are they branded? Can any be switched? Review the BNF exception list. Talk to your pharmacist-they know which generics cause substitution issues. And next time a patient asks why you switched them, explain it clearly. You’re not just saving money. You’re making care more reliable, safer, and more sustainable.


















Andrew Forthmuller
12 Nov 2025 at 21:08Generic drugs work. Period. Stop overthinking it.