

Ever opened a prescription bottle and stared at the label like it was written in code? Dosage instructions on your pill bottle or liquid medicine container aren’t just filler text-they’re life-or-death directions. Misreading them can lead to overdoses, missed doses, or dangerous side effects. And you’re not alone. A 2023 FDA report found that nearly half of all medication errors tied to prescription labels came from confusion over when and how often to take your medicine. This isn’t about being careless. It’s about unclear labeling-and how you can cut through the noise.
What Do ‘Twice Daily’ and ‘Every 8 Hours’ Really Mean?
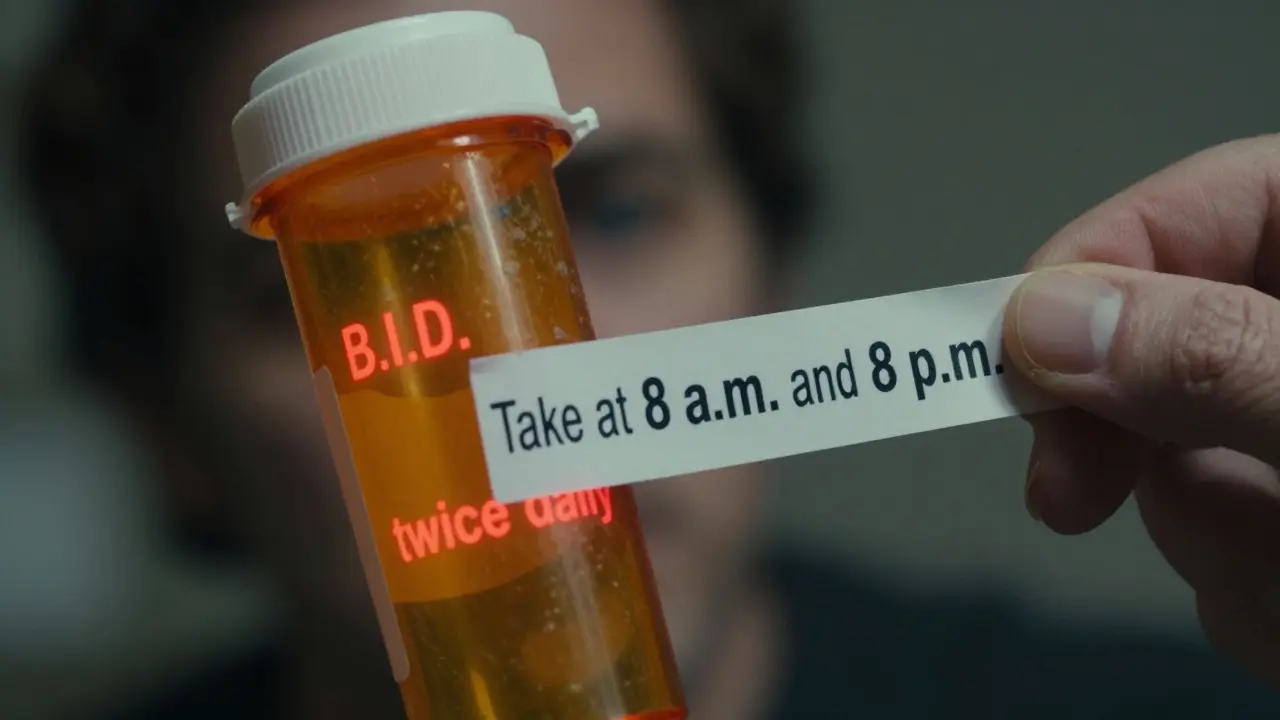
You’ve probably seen phrases like ‘take twice daily’ or ‘take three times a day’ on your label. Sounds simple, right? But here’s the catch: those terms are outdated and dangerously vague. The FDA stopped recommending them in 2014. Why? Because they don’t tell you when to take the medicine. Taking a pill at 8 a.m. and then again at 11 p.m. isn’t the same as taking it at 8 a.m. and 8 p.m. Your body’s chemistry, digestion, and sleep cycle all depend on timing.Modern labels should say: ‘Take 1 tablet with breakfast and 1 tablet with dinner.’ That’s specific. It ties the dose to a daily routine you already have. Studies from Massachusetts General Hospital show patients who got this kind of instruction were 34.7% more likely to take their medicine correctly. That’s not a small boost-it’s the difference between your treatment working and it falling apart.
But here’s the problem: most pharmacies still use the old terms. A 2023 study found 82.7% of retail pharmacy labels said ‘twice daily’ instead of giving exact times. CVS got it right 93% of the time after updating their system in 2022. Walgreens? Only 37.8%. Independent pharmacies? Barely 28%. If your label says ‘twice daily,’ ask your pharmacist: ‘Can you write out exactly when I should take this?’
Why ‘mL’ Matters More Than ‘Teaspoon’
Liquid medicines are especially tricky. Older labels might say ‘take one teaspoon.’ But a teaspoon isn’t a teaspoon. Your kitchen spoon? It holds anywhere from 3 to 7 milliliters. The FDA’s own audit of 1,247 prescriptions found that 63.8% of liquid medicine labels still used ‘teaspoon’ or ‘tablespoon.’ That’s a recipe for error.Since 2020, the National Council for Prescription Drug Programs has required all oral liquid medications to use milliliters (mL) on the label. Why? Because a 5 mL measuring cup is standardized. It’s the same every time. If your bottle says ‘take 10 mL,’ use the dosing cup that came with it-not a spoon. If no cup came with it, ask the pharmacy for one. They’re required to give it to you.
And never guess. A 2022 study in the Journal of General Internal Medicine found patients who used household spoons to measure liquid medicine made errors 27.4% of the time. That’s more than 1 in 4 doses. Even small mistakes with antibiotics, seizure meds, or pediatric syrups can cause serious harm.
What ‘As Needed’ Really Means (And What It Doesn’t)
‘Take as needed for pain’ sounds flexible. But that flexibility can kill. The FDA reports that 18.2% of preventable drug errors come from vague ‘as needed’ instructions without a daily maximum. If your label says ‘take 1 tablet as needed for pain,’ you might assume you can take it whenever you feel discomfort. But what if the maximum safe dose is 4 tablets in 24 hours? You could easily take 6 without realizing it.Consumer Reports surveyed 1,512 adults and found 67.8% didn’t know the daily limit for common pain relievers labeled ‘as needed.’ That’s terrifying. Always ask: ‘What’s the maximum number of doses I can take in a day?’ Write it down. Stick it to your fridge. For example, if you’re taking acetaminophen, the absolute max is 3,000-4,000 mg per day depending on your liver health. That’s usually 6 pills of 500 mg each. If your label doesn’t say it, demand clarity.
Timing Isn’t One-Size-Fits-All
Some medications need to be taken on an empty stomach. Others must be taken with food. Levothyroxine, for example, is absorbed poorly if taken with coffee, calcium, or iron. The FDA-approved label says: ‘Take on an empty stomach, at least 30 minutes before breakfast.’ But a Harvard Health Letter study found 32.7% of patients took it with food because they didn’t know better.For time-sensitive drugs like insulin, blood pressure pills, or chemotherapy agents, timing isn’t just helpful-it’s critical. The FDA’s Oncology Center of Excellence now requires labels to say things like: ‘Take between 8:00-10:00 a.m.’ because even a two-hour delay can reduce effectiveness. If your drug falls into this category, set two alarms: one 15 minutes before, and one at the exact time.
But what if you work nights? A 2022 Northwestern University study found 22.3% of night-shift workers got confused by ‘morning’ and ‘evening’ instructions. If you work 11 p.m. to 7 a.m., ‘take with breakfast’ doesn’t work. Talk to your pharmacist. They can adjust the timing to match your schedule. ‘Take with your first meal of the day’ is just as effective-if not more so-than forcing it into a 9 a.m. slot.
Abbreviations Like ‘B.I.D.’ and ‘T.I.D.’ Are Outdated
You might still see ‘b.i.d.’ or ‘t.i.d.’ on older labels. That’s Latin for ‘twice daily’ and ‘three times daily.’ Sounds professional, right? But the American Medical Association says only 37.4% of patients understand these abbreviations. That’s less than 2 in 5 people. The FDA banned them from patient-facing labels in 2021. If you see them, ask your pharmacist to translate them into plain English.And don’t assume ‘daily’ means ‘every day.’ Some medications are meant to be taken every other day, or only on weekdays. Always check: ‘Is this taken every day, or just on certain days?’ If the label doesn’t say, it’s not clear enough.

What’s Changing in 2024 and Beyond
The system is slowly fixing itself. Starting January 1, 2024, every new drug application submitted to the FDA must include explicit timing instructions on patient labels. That means no more ‘twice daily.’ Just ‘Take one tablet at 8 a.m. and one at 8 p.m.’California went even further with Senate Bill 1333, effective January 2024. Now, all prescription labels in the state must include both exact timing and pictograms-simple icons showing a clock and a pill, with arrows indicating when to take it. Other states are following. By 2026, the U.S. Department of Health and Human Services wants 90% of pharmacies to use this format.
And it’s not just text. The FDA is testing augmented reality labels. Scan your bottle with your phone, and a 3D animation shows you exactly when to take your medicine-complete with a clock and a visual of your stomach lining. In trials, this cut timing errors by over 50%.
Your Action Plan: 5 Steps to Avoid Medication Errors
- Read the label out loud. If you don’t understand it, say so. Ask your pharmacist to explain it in plain English.
- Replace vague terms. If it says ‘twice daily,’ ask for: ‘Take at 8 a.m. and 8 p.m.’
- Use the right tool. For liquids, use the dosing cup. Never use a kitchen spoon.
- Set phone alarms. Even if the label says ‘with meals,’ set alarms for breakfast and dinner. Your memory isn’t reliable.
- Ask the daily max. For ‘as needed’ meds, always ask: ‘What’s the most I can take in 24 hours?’ Write it on the bottle.
Medication errors aren’t about being dumb. They’re about bad design. The system is changing-but you still have to be your own advocate. Don’t just take the label as written. Ask. Clarify. Double-check. Your body will thank you.
What should I do if my prescription label says ‘twice daily’?
Ask your pharmacist to rewrite it in plain language: ‘Take one tablet at 8 a.m. and one at 8 p.m.’ The term ‘twice daily’ is outdated and can lead to confusion. Many pharmacies now use explicit timing, but not all do. You have the right to request clearer instructions.
Can I use a kitchen spoon to measure liquid medicine?
No. Kitchen spoons vary in size and can lead to dangerous overdoses or underdoses. Always use the dosing cup or syringe provided by the pharmacy. If none was included, ask for one. The FDA requires all liquid medications to be measured in milliliters (mL), and only the provided tool ensures accuracy.
What does ‘take on an empty stomach’ really mean?
It means take the medication at least 30 minutes before eating, and wait at least 2 hours after eating before taking it again. Some drugs, like levothyroxine or certain antibiotics, are absorbed poorly if taken with food, coffee, or supplements. Always check the label for specific instructions and ask your pharmacist if you’re unsure.
Why are abbreviations like ‘b.i.d.’ still on some labels?
They’re being phased out, but you may still see them on older prescriptions or in electronic records that haven’t been updated. The FDA and AMA recommend avoiding them entirely because fewer than 4 in 10 patients understand them. Always ask your pharmacist to translate them into plain English: ‘b.i.d.’ means ‘twice a day,’ but even better, they should say ‘take at 8 a.m. and 8 p.m.’
I work night shifts. How do I follow ‘take with breakfast’ instructions?
Talk to your pharmacist. ‘Take with breakfast’ means take it with your first meal of the day, no matter what time that is. If you eat at 10 p.m. after your shift, that’s your ‘breakfast.’ The goal is consistency with your routine-not a clock. Your pharmacist can help you adjust the timing to fit your schedule safely.
Next Steps: What to Do Right Now
Go to your medicine cabinet. Pull out your most recent prescription. Read the label out loud. Do you understand every word? If not, write down your question. Call your pharmacy tomorrow. Don’t wait until you feel sick or confused. Clear instructions today prevent hospital visits tomorrow.
















David L. Thomas
11 Mar 2026 at 23:42Let’s be real-‘twice daily’ is a relic from when pharmacists assumed you had a 9-to-5 and a memory like a golden retriever. The FDA’s move to mandate explicit timing? Long overdue. I’ve seen patients miss doses because they thought ‘twice daily’ meant ‘once in the morning, once before bed.’ But if your circadian rhythm’s off-say, you’re on night shift or have insomnia-that’s not just inconvenient, it’s pharmacologically dangerous.
And don’t even get me started on ‘as needed’ without a ceiling. I had a patient take 12 acetaminophen in 12 hours because ‘it wasn’t hurting that bad yet.’ We nearly lost his liver. The system’s broken, but awareness is the first dose of the cure.
Also, ‘b.i.d.’? That’s Latin for ‘we didn’t care enough to write it plainly.’ If you’re a pharmacist and you still use that, you’re not helping-you’re gatekeeping.
Good on California for the pictograms. A clock + pill icon is universal. No translation needed. If we can teach toddlers to recognize a stop sign, we can teach adults to recognize a dosing schedule.
And yes, I’m that guy who brings his own dosing cup to the pharmacy. I’ve seen too many people eyeball liquid meds with spoons. It’s like using a ruler to measure a cup of flour. You can do it… but why would you?